 6
|
6
|
 5
|
5
|
HDAC (histone deacetylase) is an enzyme in the body which governs many interactions, almost too many to mention. It can be thought of as a pathway that, when inhibited, unlocks many other pathways and increases their potency. That is true for cognitive pathways and also physical ones.
There are 10 subtypes of HDAC (excluding sirutins), and they each have a different relevance for certain bodily disorders. There exists inhibitors of all HDACs (considered "unselective) or inhibitors of specific subtypes (such as HDAC3, HDAC5 etc.), however for most subtypes of HDAC there aren't many good inhibitors. HDACs are a hard pathway to target due to their binding morphology, so avoiding toxicity while creating a selective inhibitor is hard.
For this reason most use cases involving HDAC-inhibition involve pan-HDAC inhibitors (inhibition of all subtypes). For our use cases this is also what will be useful but as they aren't selective to subtypes they can come with side effects when used.
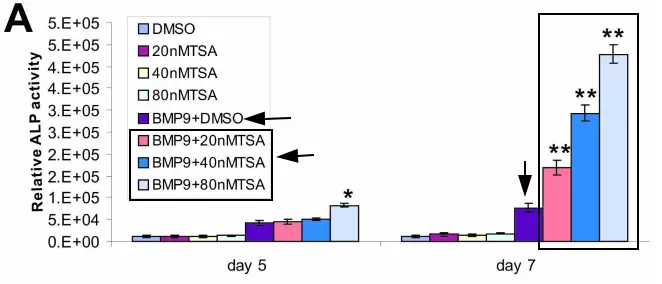
One study on BMP-9 (highly chondrogenic [cartilage forming] and osteogenic [bone forming] endogenous protein) found that simultaneous application with a pan-HDAC inhibitor increased the growth by a significant amount to the point where it made BMP-9 on its own look insignificant.
In a comparison of ALP levels (An enzyme essential for bone mineralization and growth, acting as a key marker of bone-forming cell activity), Trichostatin A (HDAC inhibitor) significantly increased expression levels:
It also significantly enhanced bone formation in a test (not directly applicable to joint models but is useful for extrapoliation):
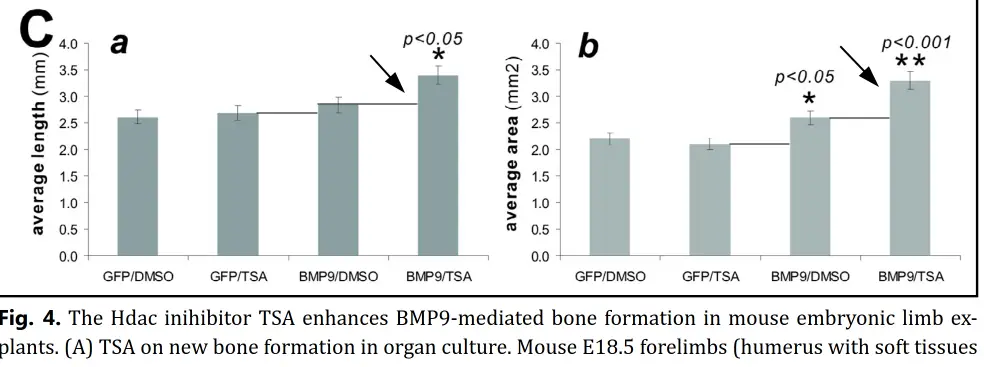
As we can see above, the combination of the osteogenic factor (BMP9) plus HDAC inhibition (the "unlocking" factor), it led to a high rate of bone growth that was not possible with the BMP alone.
In addition, on its own, pan-HDAC inhibition increases another bone morphogenetic protein, BMP-7, which is highly potent:
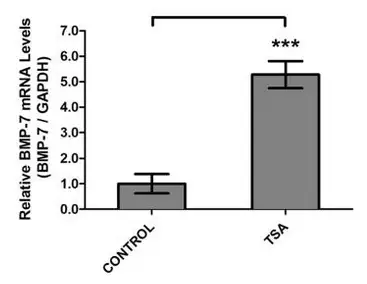
HDAC Proteins Repress BMP-7 mRNA Expression so inhibition of HDAC removes that repression.
This also applies for BMP-2 (the most osteogenic BMP): "Inhibition of HDAC increases Runx2 acetylation, and potentiates
BMP-2-stimulated osteoblast differentiation and increases bone
formation."
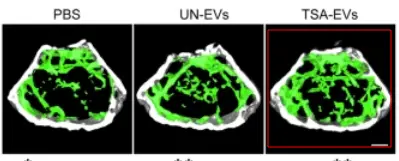
HDACi also increases bone mineral density (BMD):

This means that we can utilize the HDAC pathway for the purposes of bone growth. It has the potential to be especially useful in late puberty to after puberty. If combined with androgenic agents that increase dimorphism, and other bone growth agents (but be careful not to reduce cartilage too much otherwise it could cause issues), it could lead to very potent bone growth (appositional, BMD, endochondrial) including in the face.
HDAC inhibition alone isn't likely to increase height in adults (for many reasons I can't cover here), at least on its own. In adults it is most likely to increase bone mineral density and potentially facial bone mass, even after puberty, if combined with androgenic compounds.
POV: you use PTH analogues + HDAC inhibition + BMPs + Testosterone
There are definitely some things to be aware of. The first is that as pan-HDAC inhibitors are unselective by design (or by lack of design), they are predisposed to more side effects. There is a level of individual variance to the reaction due to CYP affinity and some other common molecular issues, alongside variance in the pathway itself.
Vorinostat (AKA "SAHA"): Most tested, FDA approved, relatively potent, poor half life. Dosed <400 mg orally.
Panobinostat: FDA approved, very potent, long half life. Dosed <20 mg orally.
Note on dosages: The ideal dose is likely lower than clinically used as we want it to be a potentiating factor rather than use it on its own. For that reason side effects will also likely be less impactful and more tolerable. Also if younger, side effects generally occur less (side effect testing is typically done on older people).
Typical side effects are listed below (roughly ordered by occurance rate):
These aren't huge concerns for these at lower doses though diarrhea (even mild) and fatigue could still be expected. If any side-effects are not manageable then use of the compound can be stopped. It is very rare for there to be any lasting negative effects mechanistically. For the use of bone growth, too much cartilage conversion also needs to be considered.
I'm personally going to be using a low dose of a HDACi (likely Vorinostat) just around when I do my injections for my height growth stack.
Hope you enjoyed the thread.