 10
|
10
|
 6
|
6
|
Table of Contents
What is Upper Eyelid Exposure (UEE)?
Why Minimize UEE? (Aesthetics, Youthfulness, and Functional Aspects)
What We Want to Achieve by the End of This Guide
Tiered System for UEE Minimization Methods
Top Tier: Surgical Options (Most Permanent & Dramatic)
Mid/Advanced Non-Surgical: Energy-Based + Regenerative
Experimental/Adjunctive Combinations (Lower Evidence)
Basic/Training Drills
What is Upper Eyelid Exposure (UEE)?
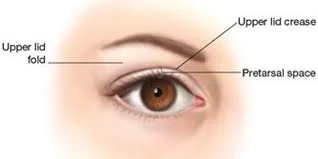
Upper eyelid exposure refers to the visible amount of the upper eyelid platform (the skin between the crease and the lash line) when your eyes are fully open, viewed from the front (frontal facial profile) or slightly angled views.
In cases of low UEE (desired in many aesthetic contexts): The upper eyelid skin appears partially or mostly "hidden" or covered by a gentle fold/hood from the brow bone or excess skin/fat. This creates a more closed, almond-shaped, youthful, and rested eye appearance. The supratarsal crease (eyelid fold) sits lower or is softer, and the eyelid platform show is minimal.
In cases of high/excessive UEE: More of the eyelid skin is visibly exposed, often making the eyes look rounder, more "open," startled, hollow/skeletal (especially with orbital fat loss), or aged in certain contexts. This can result from a high crease, retracted or weak supporting structures, fat atrophy, or post-surgical changes.
Key anatomical factors influencing UEE:
Supraorbital rim projection and brow position: A more projected (forward) brow bone/orbital rim pushes upper eyelid fat forward, increasing hooding and reducing visible eyelid exposure.
Upper eyelid fat pads: Larger, fuller pads (youthful trait) help cover the platform; atrophy increases exposure and hollowing (A-frame deformity).
Skin elasticity and dermatochalasis: Aging causes loss of collagen/elastin → excess skin that can either hood (reduce exposure) or, if combined with fat loss, create a more exposed/sunken look.
Levator muscle function: Weakness leads to true ptosis (drooping lid margin), which can paradoxically alter exposure depending on compensation (e.g., brow raising).
Orbital volume: Overall fat/bone support around the eye socket.
Genetics, aging (thinning skin, muscle weakening), sun damage, smoking, contact lens wear (long-term), significant weight loss/illness, or previous surgeries can all influence it. In aesthetics communities, minimal UEE is often preferred for a "youthful" or "hooded" eye shape, while excessive exposure can sometimes read as less rested or overly "made-up friendly" but skeletal.
Visual cue: Imagine looking straight on — if you see a lot of flat eyelid skin between lashes and crease without much overhanging fold, that's higher UEE. The opposite (soft hooding) is what many aim for when "hiding" UEE.
Importance of Addressing UEE
Minimizing excessive upper eyelid exposure can:
Create a more youthful, rested, and harmonious eye appearance (hooded eyes often signal youth and vitality due to fuller orbital support).
Improve facial balance — eyes look less "hollow" or "startled."
In some cases, enhance peripheral vision or reduce compensatory brow strain.
Boost confidence in photos/front-facing views, where eye shape heavily influences perceived attractiveness.
However, balance is key. Too much hooding can make eyes look smaller or tired. The goal is harmonious minimal-to-moderate exposure, not zero. Always prioritize function (vision) over pure aesthetics. Consult an oculoplastic surgeon for personalized assessment, as underlying ptosis or dry eye issues must be ruled out.
What We Want to Achieve by the End of This Guide
By the end, you'll understand:
The biomechanics and causes of UEE.
Evidence-based and speculative methods to reduce visible upper eyelid platform show (increase hooding/soft coverage or restore volume/support).
A clear tiered ranking of methods from most effective/permanent (surgical) to supportive/experimental.
Realistic expectations, risks, mechanisms, and how to combine approaches safely.
Emphasis on safety: Many methods here are off-label, experimental, or require professional supervision. Peptides, devices, and injectables carry risks (e.g., regulatory status, side effects). Always consult qualified medical professionals.
Tier System Legend (as expanded from your structure):
Rank 1: Highest impact, most permanent (typically surgical).
Loading/Combination tiers: Synergistic non-invasive stacks for skin tightening, volume, and regeneration.
Lower tiers: Supportive, training-based, or highly experimental with limited direct evidence for UEE.
Tiered Methods for UEE Minimization (Hiding/Reducing Exposure)
Top Tier – Surgical (Most Effective for Structural Change)
These directly address excess skin, muscle position, or hooding.
Upper Blepharoplasty for UEE Removal (often Rank 1 or 2 depending on case):
This is the gold-standard cosmetic procedure. It removes excess skin, muscle, and sometimes fat from the upper eyelids through an incision in the natural crease. Result: Reduced hooding in cases of dermatochalasis, smoother platform, but it can actually decrease excessive exposure by tightening and reshaping if the issue is laxity creating unnatural show. It creates a more defined yet rested look and can be combined with fat repositioning or conservative removal to avoid hollowing.
Mechanism: Excises redundant tissue, allowing better draping and reducing visible platform when hooding is the goal or when over-exposure stems from stretched skin. Outpatient, local anesthesia, recovery 1-2 weeks (swelling/bruising).
Ideal for age-related sagging or genetic excess skin. Risks: Over-resection (hollow eyes), asymmetry, dry eye. Often preferred when the primary complaint is "heavy" lids impacting aesthetics or vision.
Upper Blepharoplasty (general/rank 2 variant): Similar to above, focused on hooding correction by removing sagging skin/fat that causes the "hooded" look. It improves the eyelid contour for a youthful, open-yet-covered appearance. Can be tailored conservatively to enhance subtle hooding rather than fully "opening" the eye.
Ptosis Surgery for UEE Adjustment (Rank 3):
Corrects true drooping of the eyelid margin due to levator muscle/aponeurosis weakness or stretch. Techniques: External (incision in crease, tighten levator) or internal (Müller’s muscle resection, no visible scar).
Mechanism: Repositions the lid margin higher or lower as needed, directly controlling how much platform is exposed. In over-exposed cases (high lid position), it can subtly lower the margin for more coverage. Often combined with blepharoplasty.
Functional benefits (better vision) + cosmetic. Recovery similar to bleph. Risks: Over/under-correction, lagophthalmos (incomplete closure). Best when muscle weakness contributes to abnormal exposure.
Hooding Bleph (Rank 4 – Targeted Upper Lid Blepharoplasty):
Specifically excises excess, sagging skin/fat causing "hooding" over the crease/lashes. This can paradoxically help control exposure by reshaping the fold for optimal coverage without fully eliminating the youthful hooded quality. Common in aging patients; creates a crisp yet soft transition.
Note on ranking: Pure "UEE removal" (reducing high exposure) often favors ptosis repair + conservative bleph to lower/reshape the lid position and restore volume support. Full hooding-focused bleph increases coverage. Choose based on your specific anatomy (consult oculoplastics).
Mid/Advanced Non-Surgical: Energy-Based + Regenerative Combinations
These aim to tighten skin, boost collagen, restore volume, and support tissue for gradual reduction in excessive exposure or improved hooding d(R)@pe.
Exposure-Reducing PEMF Skin (Base Loading) + PEMF Technology:
Pulsed Electromagnetic Field (PEMF) therapy uses low-frequency electromagnetic waves to stimulate cellular repair. Non-invasive, applied via devices/mats/pads.
Mechanism for skin/eyelids: Improves microcirculation, reduces inflammation, enhances ATP production, and promotes fibroblast activity leading to increased collagen and elastin synthesis. This can tighten lax periorbital skin, improve elasticity, and support better tissue "d(R)@pe" over the eyelid platform (potentially reducing unnatural exposure by firming without hollowing). Studies show benefits in skin rejuvenation, laxity reduction, and wound healing when combined with RF. Safe for facial use; sessions are relaxing.
How to use for UEE: Targeted periorbital applicators or full-face protocols, multiple sessions. Combine as "loading" base for other treatments. Limitations: Subtle results; not a replacement for surgery in severe cases. Evidence is growing but stronger for general skin tightening than specific eyelid exposure.
Exposure-Reducing PEMF + Volufiline:
Add Volufiline (sarsasapogenin from Anemarrhena asphodeloides), an oil-soluble cosmetic ingredient claimed to stimulate adipocyte (fat cell) differentiation and lipid accumulation.
Mechanism: Topical "plumping" via increased fat storage in subcutaneous tissue. Applied as serum/oil to periorbital/upper lid area. May help restore subtle volume to hollowed or exposed lids, supporting more natural hooding and reducing skeletal show. Popular in eye creams for under-eyes/temples; some anecdotal reports for upper lids. Oil-based formulas penetrate better.
Synergy with PEMF: PEMF enhances circulation/collagen while Volufiline targets volume. Consistent daily use (weeks to months) + PEMF sessions. Evidence: Limited clinical trials; mostly manufacturer data and user reports. Safe topically but results vary; not dramatic like fillers.
Red Light Therapy (Upper Eyelids) + BPC-157:
Red/Near-Infrared Light Therapy (RLT, ~630-830nm): Uses LED devices to penetrate skin.
Mechanism: Stimulates mitochondrial cytochrome c oxidase → increased ATP, collagen/elastin production by fibroblasts, reduced inflammation, improved circulation. For eyelids: Tightens delicate skin, reduces fine lines/laxity, may subtly lift/support for better coverage. Safe for periorbital area with eye protection; home devices or clinical sessions. Studies support facial skin tightening and post-bleph healing.
BPC-157 (Body Protection Compound-157): Synthetic peptide from gastric juice. Administered orally, topically (creams), or subcutaneously (under medical guidance).
Mechanism: Potent regenerative/anti-inflammatory effects; upregulates growth factors, angiogenesis (new blood vessels), and collagen synthesis. May accelerate tissue repair, improve skin elasticity, and support youthful glow in periorbital area. Animal studies show wound healing benefits; human use is off-label/experimental for aesthetics.
Synergy: RLT boosts cellular energy while BPC aids repair/collagen. Potential for improved eyelid skin quality and subtle volume/support. Risks: Peptides require sourcing/medical oversight (not FDA-approved for this). Start low-dose.
Ultrasound Upper + Pearl: This appears to reference high-intensity focused ultrasound (HIFU) or micro-focused ultrasound (e.g., Ultherapy) for skin tightening around the upper eyelids/brow. It delivers focused ultrasound energy to heat deep layers, contracting collagen and stimulating new formation for lifting/tightening. "Pearl" may allude to treatment pearls or protocols. Can provide non-surgical brow lift effect, indirectly reducing exposure by improving support. Evidence: Good for mild laxity; multiple sessions needed. Combine cautiously with other modalities.
Experimental/Adunctive Combinations (Lower Evidence/Base Support)
These are more speculative or supportive:
Enema + Needling Upper: Unclear direct link. Enemas relate to gut detox/hydration (systemic inflammation reduction may indirectly benefit skin via gut-skin axis). "Needling upper" likely means microneedling or acupuncture/dry needling around upper eyelids/periorbital area to stimulate collagen, improve circulation, and tighten. Microneedling creates micro-injuries triggering repair. Limited specific evidence for UEE; more general skin rejuvenation. Not a core method—use as adjunct under professional care. Risks: Infection, irritation in delicate eye area.
Raw Eggs + TENS: Highly experimental/anecdotal. Raw eggs (topical?) for proteins/nutrients or internal for nutrition (biotin, etc., supporting skin/hair). TENS (Transcutaneous Electrical Nerve Stimulation): Uses mild electrical currents for pain relief or muscle stimulation. Could theoretically tone orbicularis/levator muscles if applied carefully (not standard for eyelids). No strong evidence for UEE reduction; potential for irritation. Approach with extreme caution or skip—better alternatives exist.
Basic/Training Drills
Pinhole + Blackout Drills:
Pinhole: Using pinhole glasses or exercises (looking through small apertures) to train eye muscles/focus, potentially improving control over lid position or reducing strain.
Blackout drills: Likely sensory deprivation or eye patching/blackout training to strengthen muscles or awareness of lid posture (similar to vision therapy or mewing-adjacent drills in aesthetics communities). May help with compensatory habits (e.g., brow raising) or subtle muscle tone. Low risk, zero cost; benefits are indirect (better overall eye health/awareness) rather than structural volume/skin change. Consistent daily practice (minutes) as maintenance.
Final Advice for Implementation
Start conservative: Assess your anatomy (photos, consultation). Address lifestyle first (sleep, sun protection, no smoking, hydration, nutrition).
Stack intelligently: Use PEMF/RLT as foundation + topicals like Volufiline + peptides (supervised) before considering surgery.
Realistic timelines: Non-surgical: 4–12+ weeks for subtle changes. Surgical: Immediate but swelling resolves over months.
Risks & Professional Input: Surgery has downtime/risks (scarring, asymmetry, dry eye). Devices/peptides: Variable regulation. Never self-experiment aggressively around eyes.
Monitoring: Track progress with consistent frontal lighting photos.
This guide prioritizes truth-seeking: Surgical options have the strongest evidence for significant change, while non-invasive stacks offer supportive, lower-risk improvements via collagen/volume pathways. Combine methods synergistically for best results, but individual response varies widely due to genetics and age. If you have specific photos, anatomy details, or want protocols/dosages expanded, provide more info for further tailoring. Consult specialists (oculoplastic surgeon, dermatologist) before any intervention.
TAGS: @ @
@ @
@ @
@ @
@ @
@ @
@