 6
|
6
|
 2
|
2
|
Why do people call it cope?
The main reason GH analogs are often called cope is because people look at the serum IGF-1 levels and then compare it to HGH as if its a fair comparison
Why is this wrong?
Serum IGF-1 is not the only IGF-1, it is just the one that’s tested in blood test etc.
So why are they not cope?
GH analogs(specifically ones that mimic natural patterns) increase skeletal IGF-1 aka local IGF1
This skeletal/local IGF-1 is actually protective of growth plates, it is responsible for the actual tissue, cells, growth plate, etc.
in this study, they compared pulsatile GH administration to to a continuous infusion of GH.
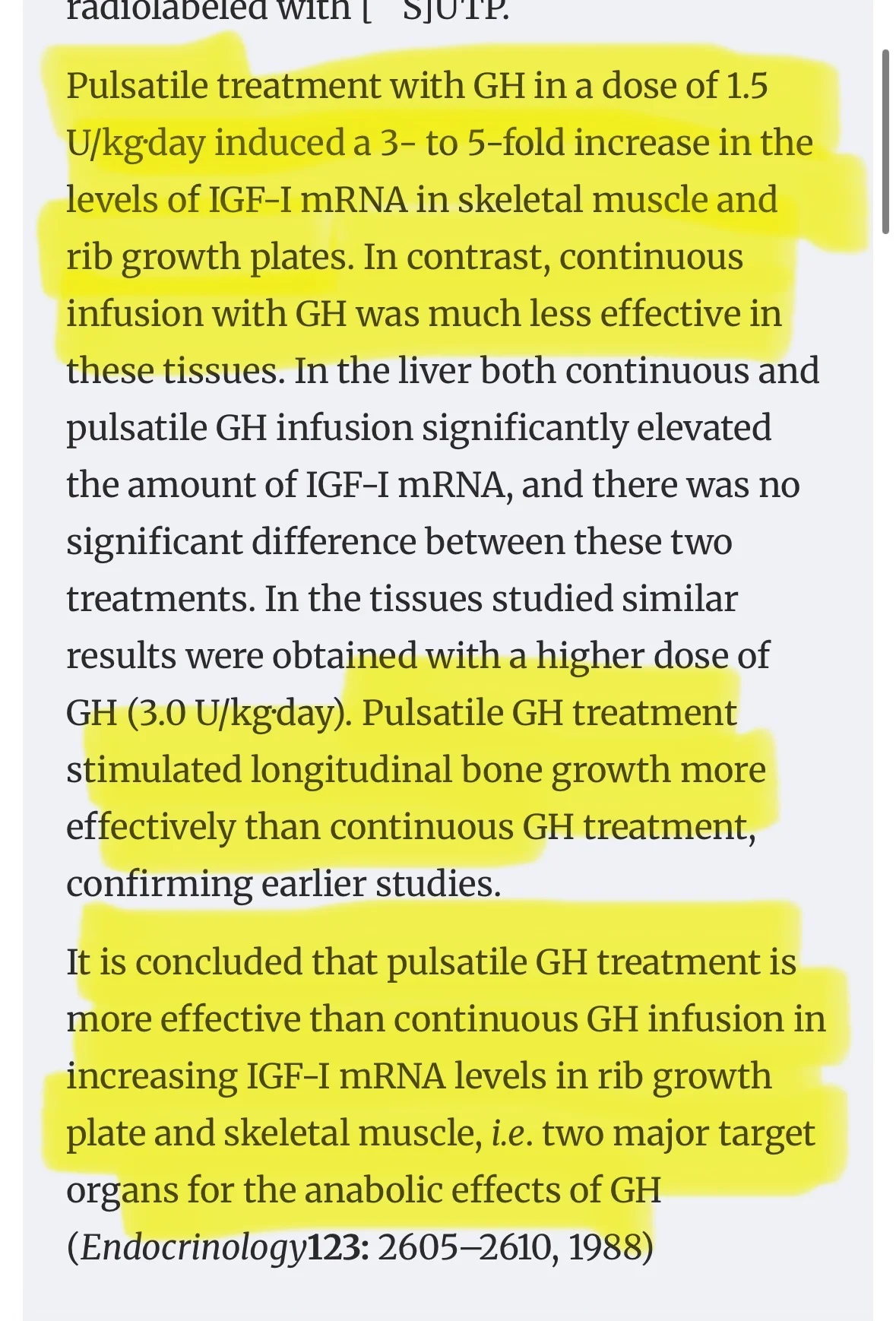
this has been shown in many studies
TLDR: Pulsatile GH treatment increased skeletal/local IGF-1 far greater than a continuous infusion. Not only this but this pulsatile GH treatment was also more effective at stimulating longitudinal bone growth.
https://pubmed.ncbi.nlm.nih.gov/8603568/
this study is important since it also compared a mixed treatment. It includes the pulsatile vs continuous as well as a pulsatile + continuous
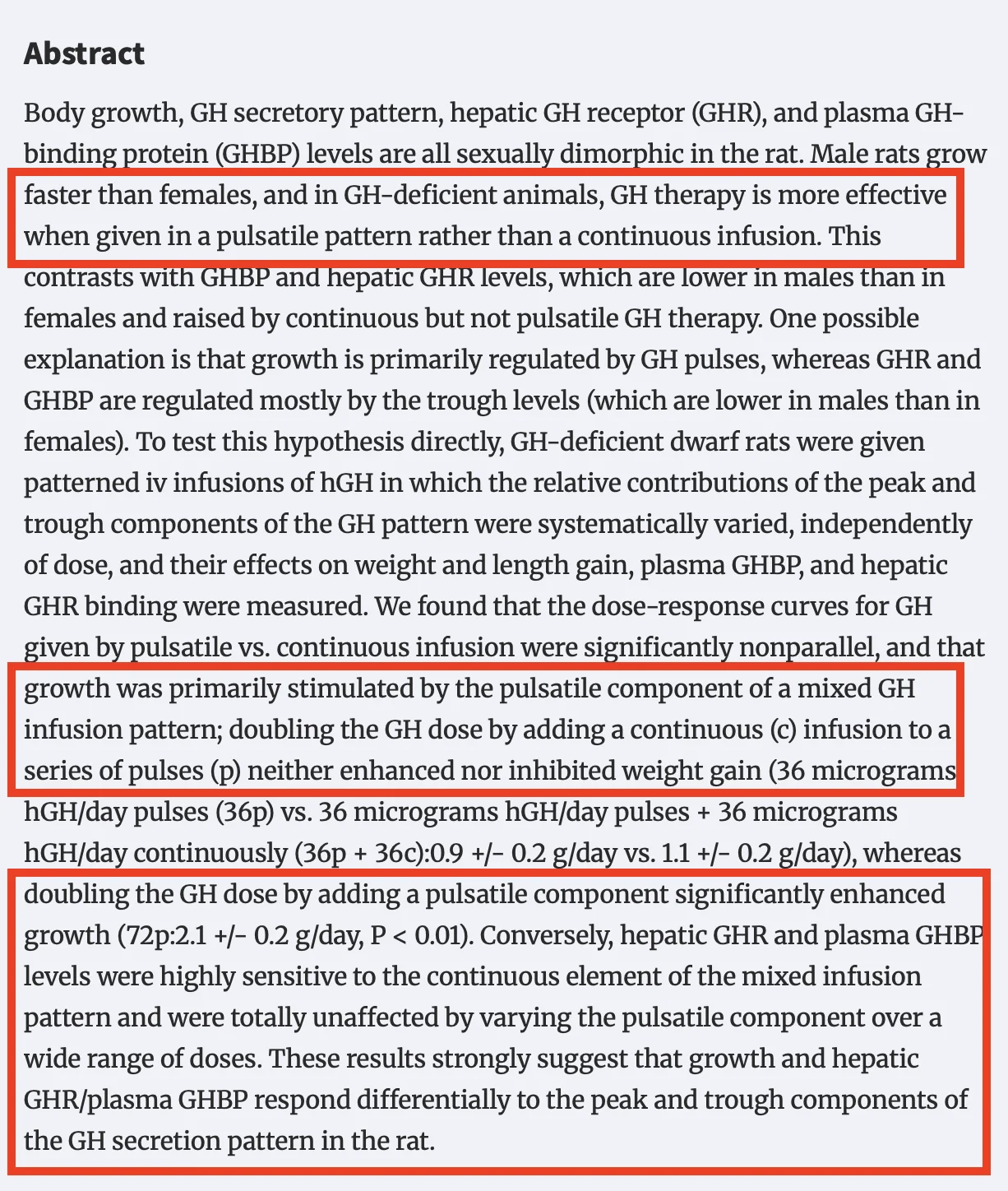
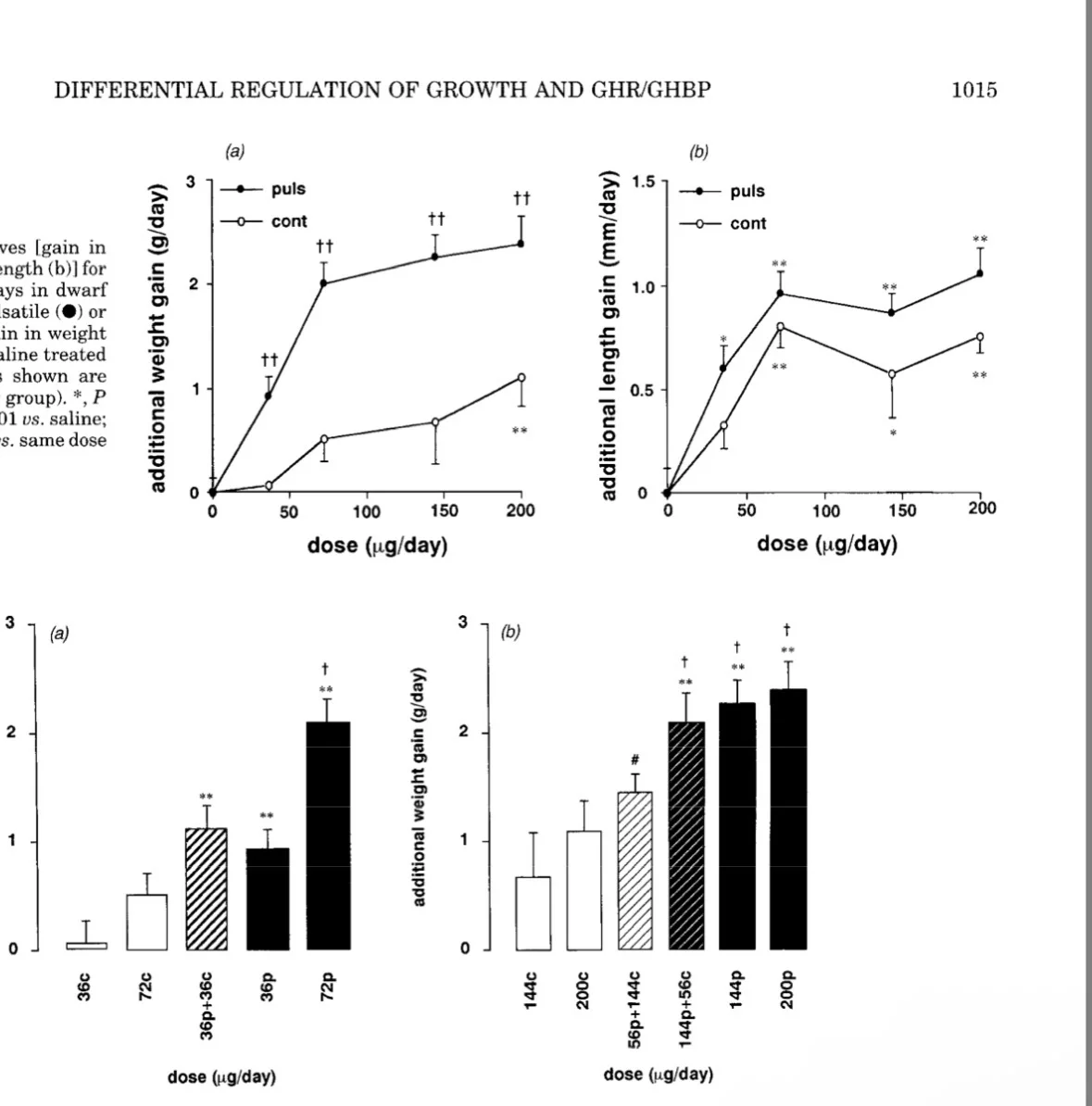 R: This shows that pulsatile GH is much more effective for longitudinal growth etc. When pulsatile GH infusions were added to the continuous group, growth increased a ton however when continuous GH was added on top of pulsatile GH infusions there was no extra growth even when added on top/doubled dose.
R: This shows that pulsatile GH is much more effective for longitudinal growth etc. When pulsatile GH infusions were added to the continuous group, growth increased a ton however when continuous GH was added on top of pulsatile GH infusions there was no extra growth even when added on top/doubled dose.
also a quick note, this does not mean serum GH is useless, its obviously crucial, its sort of just "incomplete"
WHAT TO LOOK FOR:
We want to look for GH peptides that specifically increase pulses and cause sharp pulses. avoiding things that focus on serum GH since this will create a "flattened" profile which may decrease the effect of Pulsatile GH(not confirmed).
What's optimal:
Ipamorelin - ipamorelin is one of the best peptides for skeletal GH since it actually increases Pulsatile GH and causes sharp pulses rather than just increased serum GH.
GHRP-2 - also one of the best for skeletal GH since it also increases pulsatile GH and it even increases the actual burst mass itself, however, it also increases serum GH which may cause a "flattened" profile(effects not confirmed) + it can increase cortisol

Mid Tier:
CJC-1295 no dac- cjc even without dac is still not optimal. It only really preserves the natural GH pulses rather than "increasing" them, and it also increases serum GH quite a lot meaning it could be a "flat profile". also make sure if u use it its no dac(if it has dac it wont preserve natural pulses so it does fucking nothing)
Tesamorelin - again, yes it raises serum levels but it doesnt really increase natural pulses or have a sharp effect
Hexalerin - extremely good about boosting Pulsatile GH however you can get desensitized quickly and it also raises prolactin/cortisol
Usable but not recommended:
MK-677 - similar issue as cjc, yes it raises serum igf1 but it doesnt have the sharp/strong added gh pulses needed, it also has prolactin/cortisol which may cancel out some of the benefits
DO NOT USE:
CJC-1295 w Dac - self explanatory, doesn't preserve natural pulses so
Other more indirect peptides etc:
Retatrutide - may create a "better environment" for GH pulses(insulin suppresses GH so by reducing it and creatign a better environment you can have larger GH pulses)
not only do they boost pulsatile GH and in tern skeletal IGF1, but they also carry MUCH lower risk then HGH, or even CJC since rhey mainly focus on enhancing pulsation rather than endocrine/serum IGF1